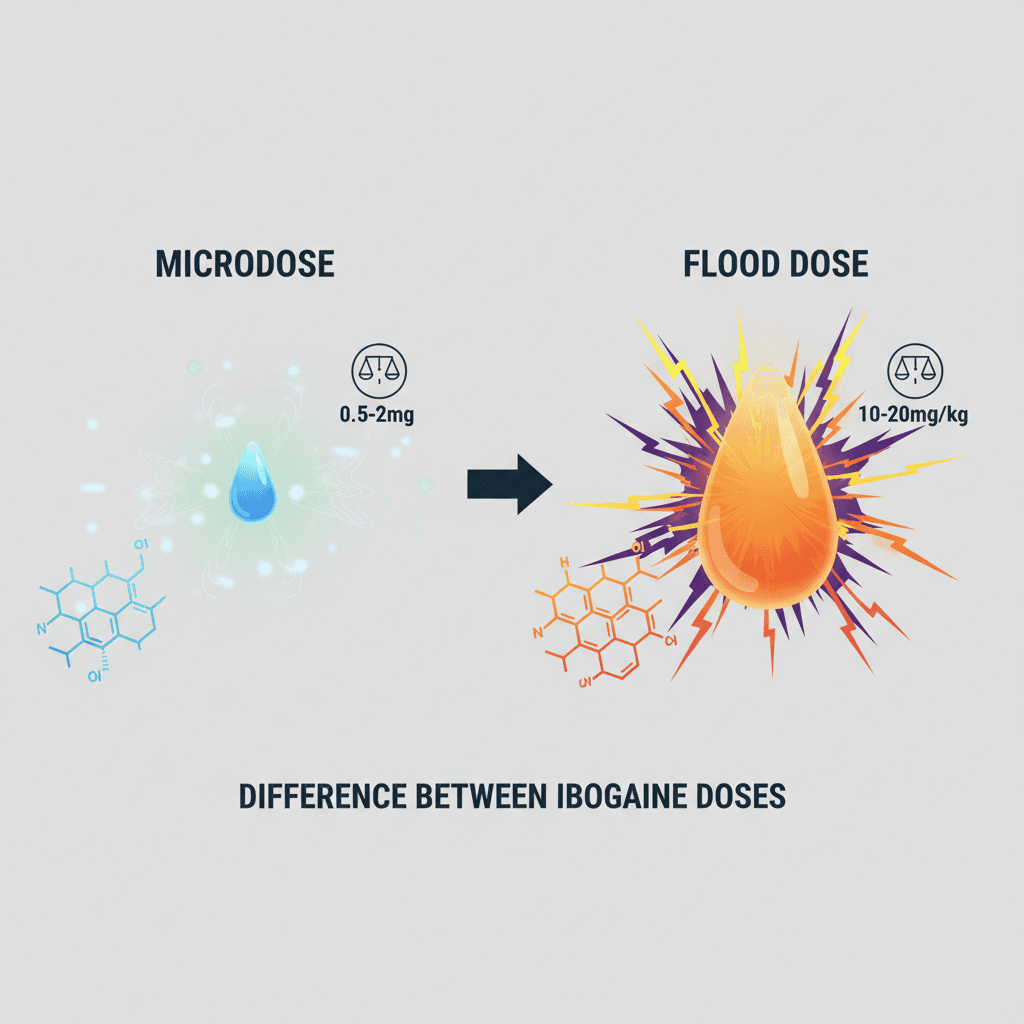
Ibogaine is not a one‑size‑fits‑all medicine. The difference between ibogaine doses, especially microdosing versus flood dosing, changes almost everything about the experience, the potential benefits, and the level of medical risk you take on.
If you are trying to understand how ibogaine is used in clinical programs compared with more experimental or self‑directed use, it helps to look closely at why different doses are used, what they are intended to do, and what the safety data tells you.
Understanding basic ibogaine dosing ranges
Before you compare microdosing and flood dosing, it is useful to know how clinicians and researchers describe different dose levels. Ibogaine dosing is usually discussed in milligrams of ibogaine per kilogram of body weight (mg/kg).
Typical ranges you will see in the literature include:
- Test dose: about 2 to 3 mg/kg to check for allergic or unusual reactions and to observe how your body metabolizes ibogaine, often used in structured protocols before a larger dose [1].
- Therapeutic / full dose: about 10 to 12 mg/kg in more conservative clinical research settings, sometimes higher in informal or non‑regulated clinics.
- Flood dose: around 15 to 20 mg/kg or more, designed to induce intense visionary states and strong interruption of withdrawal or addictive patterns [2].
- Booster dose: about 1 to 5 mg/kg, used to extend or reinforce effects after an initial dose [1].
Microdosing with ibogaine is generally far below these ranges, often at a small fraction of 1 mg/kg, and is usually repeated over days or weeks. You can explore the broader dosing landscape in more detail in ibogaine dosing methods explained.
What is a flood dose of ibogaine
Flood dosing is what most people think of when they imagine classic ibogaine treatment. A flood dose is a high, usually single, oral dose of ibogaine that aims to create a powerful, multi‑phase psychedelic experience and a rapid reset of substance use symptoms.
In one clinical setting in Mexico, patients typically received around 15 mg/kg, with some variation of plus or minus 5 mg/kg based on weight and the severity of polysubstance use [2]. At this level, a flood experience:
- Comes on after about 1 to 3 hours
- Enters a vivid visionary phase that can last 4 to 8 hours
- Moves into a reflective phase over the next 8 to 20 hours
- Gradually tapers into a residual phase that may extend 24 to 72 hours
The entire experience can last 12 to 36 hours, with lingering after‑effects for several days [2]. If you want a deeper look at what this can feel like, you can read more in what is a flood dose ibogaine and ibogaine flood dose experience.
What is ibogaine microdosing
Microdosing is essentially the opposite end of the spectrum. Instead of one large psychedelic session, you take very small, sub‑perceptual doses of ibogaine or its related alkaloids repeatedly over time.
In a microdose, you typically do not experience:
- Intense visual phenomena
- Loss of motor control
- A prolonged bed‑bound state
The goal is usually not to have a dramatic single‑night breakthrough. Instead, you are aiming for gradual shifts in mood, anxiety, cognition, or cravings over days or weeks. Programs that focus on this approach, especially for mood or functional support, often refer to ibogaine microdose therapy and ibogaine microdosing benefits.
Exact microdose amounts can vary widely and are not standardized in the way clinical flood doses are. This variability is part of why safety conversations are so important.
Core difference between ibogaine doses
When you compare microdosing and flood dosing, you are really comparing two different treatment philosophies.
In simplified terms:
| Aspect | Microdosing | Flood dose |
|---|---|---|
| Typical goal | Gradual support, mood and functioning | Rapid interruption of addiction or deep psychological reset |
| Dose size | Very low, often a fraction of 1 mg/kg, repeated | High, around 10 to 20 mg/kg, usually once in a session |
| Subjective effect | Mild or sub‑perceptual | Intense psychedelic and visionary experience |
| Duration of one session | Hours, but usually manageable in daily life | 12 to 36 hours of acute effects, up to 72 hours of residual |
| Common setting | Experimental, self‑directed, some integrative clinics | Medically supervised programs or informal treatment centers |
| Risk level per dose | Lower acutely, but cumulative exposure matters | Higher cardiac and neurological risk, requires monitoring |
Both approaches exist on the same spectrum of ibogaine dosing. The key difference between ibogaine doses here is not only quantity, but purpose, context, and safety management.
You can see how these fit together in a broader ibogaine dosage comparison or in the overview ibogaine microdosing vs flood dose.
Why clinical programs use structured dosing protocols
Medical and research programs generally avoid improvising with ibogaine. Instead, they rely on structured protocols that are built to reduce risk.
Guidance from clinical groups suggests several important safeguards:
- Using a test dose of 2 to 3 mg/kg several hours before a larger dose to detect allergic reactions and unusual metabolic responses [1].
- Adjusting mg/kg dosing for people who are significantly underweight or overweight, because digestive system size and body composition can change how ibogaine is absorbed and processed [1].
- Carefully evaluating liver function, since hepatic conditions or elevated liver enzymes can lead to rapid, prolonged, or intensified ibogaine effects. Such patients may require longer observation after a test dose, often at least eight hours before any additional dosing [1].
- Timing full dosing so that opioid withdrawal symptoms are present, but not extreme, with an Objective Opioid Withdrawal Score between 3 and 7 for optimal safety and effect [1].
- Keeping total doses at or below 12 mg/kg whenever possible, and in any case below an absolute maximum of 24 mg/kg within a 24‑hour period, due to rising cardiac risks above that range [1].
You will often see booster doses of 1 to 5 mg/kg used either shortly after the main dose, or at least 24 to 36 hours later, in order to avoid stacking peaks of cardiac stress [1].
If you are evaluating any clinical or retreat option, asking how closely they follow a formal ibogaine treatment dosing protocol can give you a quick sense of how seriously they take safety.
Safety data and concerns at different dose levels
Ibogaine is powerful, and its risk profile changes as doses increase. Understanding this helps you weigh the potential benefits against the potential harms.
High doses and cardiac risk
One controlled study in opioid use disorder patients used a 10 mg/kg single oral dose of ibogaine hydrochloride and monitored heart function over 24 hours. At this dose:
- The median maximum QTc interval increase was 95 milliseconds
- Half of participants had a QTc interval above 500 ms at some point within 24 hours
- Mild bradycardia and lowered blood pressure were common within the first 12 hours
- All participants experienced severe transient ataxia, meaning an inability to walk without support, peaking 2 to 6 hours after ingestion and resolving within 24 hours [3]
QTc prolongation is a known risk factor for serious arrhythmias. While this particular study did not observe torsades de pointes or seizures, the authors emphasized that these dose‑related cardiac effects are clinically significant and require close monitoring [3].
They also noted that QTc prolongation tended to persist in some individuals, staying above 450 ms in nearly one third of participants even after 24 hours, likely due to the longer half‑life of ibogaine’s metabolite, noribogaine [3].
Based on these findings, the researchers suggested that repeated low‑dose strategies might offer a better safety margin, provided that strict ECG monitoring and genetic testing for CYP2D6 metabolism are used to identify high‑risk individuals [3].
Toxicology and lethal dose considerations
Toxicological research in animals provides additional perspective:
- In rodents, effective ibogaine doses for some behavioral effects can also cause neuronal injury to Purkinje cells in the cerebellum, pointing to potential neurotoxicity at higher doses [4].
- The approximate oral lethal dose in rodents is about 263 mg/kg, which is far above typical human flood doses but still serves as a reference for understanding margins of safety [4].
When these animal data are converted to humans and adjusted for species differences and individual vulnerability, one analysis estimated a safe initial human dose of around 0.87 mg/kg, much lower than what many treatment centers actually use [4]. The authors warned that without reconsidering current high‑dose practices, morbidities and mortalities associated with ibogaine treatment are likely to continue.
Observational data from treatment centers
Real‑world dosing in some treatment facilities has often been more aggressive than research protocols. At the Crossroads clinic in Mexico between 2012 and 2015, typical doses were around 15 mg/kg with an adjustment of plus or minus 5 mg/kg [2].
In that observational cohort:
- Participants consistently reported intense visions and a significant reduction in acute withdrawal symptoms
- The study did not find clear differences in subjective intensity or outcomes within that 10 to 20 mg/kg range
- There was no formal dose‑response analysis to show whether more ibogaine within that band improved outcomes or only increased risk [2]
The authors called for more rigorous, controlled studies to clarify how different doses influence both efficacy and safety in opioid use and psychological outcomes [2].
Emerging work with structured lower‑risk protocols
More recent work has started to explore carefully designed protocols that may hold potential benefits at more moderate risk levels. One study of 30 veterans with traumatic brain injury and severe PTSD, depression, and anxiety used oral ibogaine combined with magnesium in a clinical setting [5].
In that group:
- Average disability scores improved from mild to moderate disability to effectively no disability one month after treatment
- PTSD symptoms decreased by about 88 percent, depression by 87 percent, and anxiety by 81 percent relative to pre‑treatment
- No serious cardiac events were reported, and side effects were mostly mild, including headaches and nausea [5]
The study, however, did not compare different doses. It reported results from a single structured regimen, so you cannot yet conclude how dose variations would affect outcomes or safety [5].
Positive and negative aspects of flood dosing
High‑dose or flood dosing often attracts attention because of its dramatic potential benefits, especially in cases of severe opioid or polysubstance dependence. At the same time, it concentrates much of ibogaine’s risk into a single intensive window.
Potential positives of flood doses
You may see the following potential advantages discussed:
- Rapid interruption of opioid withdrawal and cravings for some people, sometimes within hours
- A single, memorable experience that feels like a psychological reset
- Intense introspective and visionary content that some people describe as life‑reorganizing
- The possibility of making large changes in a short time, especially when integrated with ongoing therapy
Many treatment programs that focus on full‑dose work, such as those described in ibogaine full dose treatment, build their approach around preparing you for that one very significant experience, then supporting you in integrating what you saw and felt.
Key negatives and risks of flood doses
The same intensity that creates potential breakthroughs also brings a higher probability of medical complications. Research and clinical guidance highlight several concerns:
- Serious cardiac events such as QTc prolongation, bradycardia, and arrhythmias, especially above about 10 to 12 mg/kg [6]
- Prolonged ataxia and inability to walk without support, which can increase risk of falls or injuries in poorly supervised settings [3]
- Gastrointestinal distress, ventricular arrhythmias, and unexplained sudden deaths reported in association with high doses, especially in non‑medical settings [4]
- Potential neurotoxicity at higher doses, at least in animal models, with damage observed in specific brain cell populations [4]
If a provider does not screen for cardiac issues, does not monitor you with ECG, or ignores dose ceilings that experts recommend, the risk profile can become significantly worse.
Positive and negative aspects of microdosing
Microdosing is often perceived as gentler and safer, but it carries its own trade‑offs, especially since the research base is much smaller and less standardized.
Possible positives of microdosing
People attracted to microdosing ibogaine usually hope for:
- Better day‑to‑day functioning without losing the ability to work or care for family
- Subtle mood, anxiety, or cognitive improvements over time
- Support in gradually reducing certain substances or habits without a single intense detox
- Lower acute risk of extreme cardiac events compared with flood doses, assuming each microdose is genuinely small
Because the subjective effects at each dose are minor, many people feel more in control of pacing and daily life. Integrative approaches that explore ibogaine microdose therapy and ibogaine microdosing benefits often emphasize careful titration and ongoing medical supervision.
Limitations and potential negatives of microdosing
Microdosing has several important uncertainties:
- You may not get the dramatic interruption of addiction or compulsive behavior that flood dosing sometimes provides.
- Cumulative exposure over many days may still affect your heart, especially if you have unrecognized cardiac risk factors.
- There is no widely accepted standard protocol, which means dose size, frequency, and duration can vary significantly between practitioners or self‑directed users.
- Because effects are subtle, you may be tempted to increase your dose without proper monitoring, and that can inadvertently move you into higher‑risk ranges.
There is also much less clinical data on long‑term, repeated ibogaine exposure compared with single or few flood doses. Until these data exist, microdosing should still be approached cautiously and ideally within a structured medical context.
Choosing between different ibogaine dose approaches
If you are trying to decide between microdosing and flood dosing, it can help to ask yourself and any prospective provider some specific questions.
You might consider:
- Your primary goal. Are you aiming for a rapid reset of severe addiction, or for gradual improvements in mood and functioning?
- Your medical profile. Do you have any known heart, liver, or neurological issues? Have you had a recent ECG and liver panel?
- The setting. Will you have continuous cardiac monitoring during higher doses? Is there medical staff on site who are familiar with ibogaine’s specific risks?
- How prepared you are for integration. A flood dose can bring up a vast amount of material in a short time. Do you have therapeutic support in place to work with what emerges?
- Your tolerance for risk. Even under monitoring, higher doses carry more acute danger than very small doses. On the other hand, very small doses may not achieve the outcomes you are hoping for, especially with severe substance use.
If you want to understand in more depth how professionals structure both approaches, you can explore ibogaine dosing methods explained and ibogaine treatment dosing protocol for a broader context.
The importance of medical supervision and ongoing research
What stands out across the research is that ibogaine is both promising and hazardous. High doses have been linked with serious events including ventricular arrhythmias and sudden deaths, particularly when used without strict medical oversight [4]. Even at 10 mg/kg, which is on the lower end of flood ranges, clinically relevant QTc prolongation and severe ataxia are common [3].
At the same time, when ibogaine is used in structured protocols with careful dosing, heart monitoring, and risk reduction strategies like magnesium co‑administration, preliminary data suggest meaningful reductions in PTSD, depression, anxiety, and disability for some groups [5].
Future controlled trials are needed to answer key questions that matter for you, including:
- Whether lower, repeated doses can match the benefits of flood doses with a safer cardiac profile
- How microdosing compares directly with single high‑dose sessions for different conditions
- Which individual factors, including metabolism and medical history, should most strongly guide dose selection [2]
Until those answers are clearer, the safest path is to treat any ibogaine dose as medically significant, to prioritize settings that follow conservative dosing limits, and to be cautious about unstructured or self‑directed experimenting.
The difference between ibogaine doses is ultimately the difference between gradual, lower‑intensity support and a concentrated, high‑risk intervention. Understanding both sides helps you ask better questions, recognize red flags, and choose an approach that aligns with your needs, your health, and your tolerance for risk.