Understanding ibogaine dosage comparison
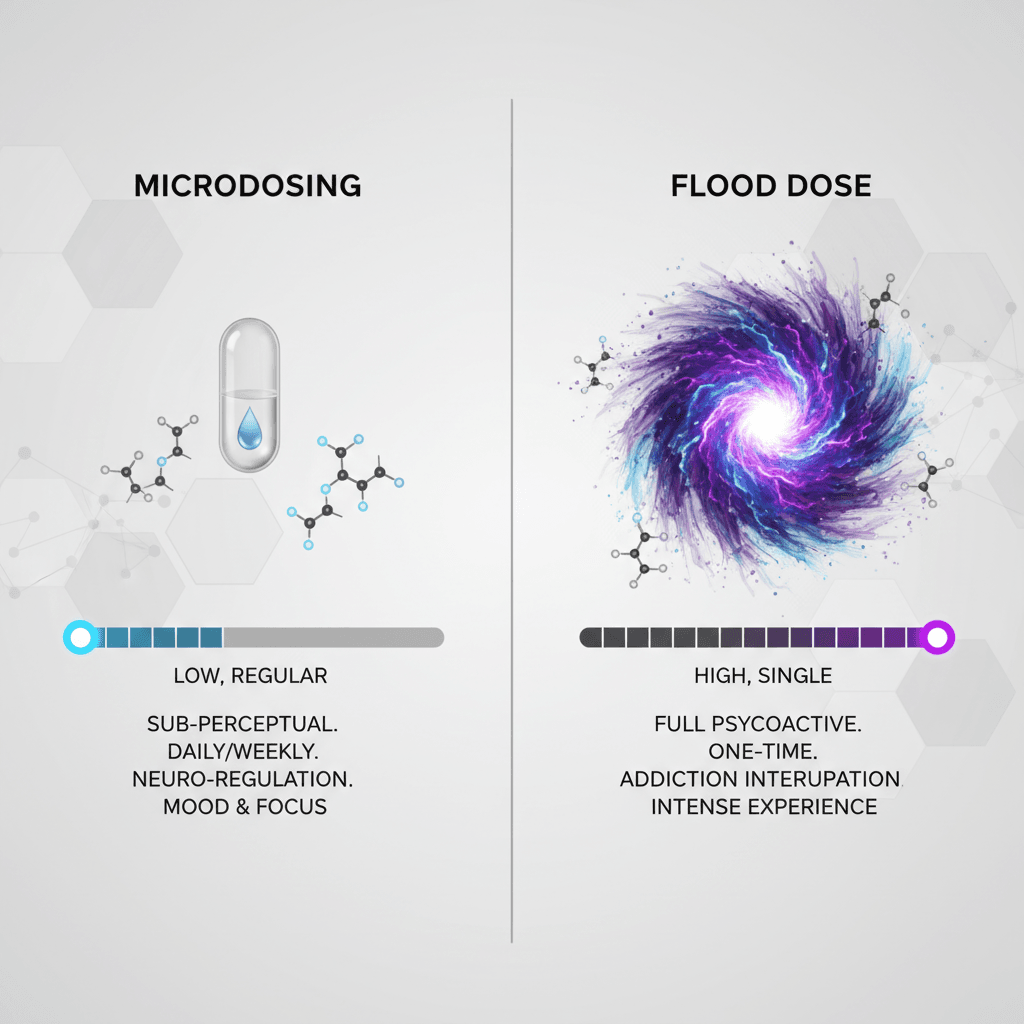
When you start looking into ibogaine treatment, you quickly discover there is no single standard dose. An ibogaine dosage comparison usually centers on two very different approaches: microdosing and flood dosing. Each method has different goals, effects, safety considerations, and levels of medical oversight.
You might see inspiring stories of people who say ibogaine eliminated withdrawal, reset their brain, or gave them life changing insights. You will also see serious warnings about cardiac risks and sudden deaths. Making sense of these mixed messages starts with understanding how ibogaine dose, setting, and protocol interact.
In this guide, you explore how microdosing compares to flood dosing, what the research says about each, and why clinical programs favor structured, medically supervised protocols instead of self-directed trial and error. Along the way you can use resources like ibogaine dosing methods explained and difference between ibogaine doses as deeper dives into specific topics.
Core ibogaine dosing ranges
Before you look at specific methods, it helps to understand the basic ranges that show up repeatedly in both research and clinical practice. Ibogaine dosage is most often described in milligrams per kilogram of body weight (mg/kg).
At a high level, you will see three broad categories:
- Microdose range
- Therapeutic or low to moderate dose range
- Flood dose or full dose range
The details within each category matter for both safety and outcomes.
Microdose and sub‑perceptual range
Microdosing typically involves very small amounts of ibogaine taken repeatedly over days or weeks. Exact microdose ranges vary across programs and self-experimenters, but they usually represent a small fraction of the doses used in addiction treatment.
With microdosing, you are aiming for:
- Little or no acute psychedelic effect
- Subtle shifts in mood, cognition, or energy
- The ability to continue normal daily activities
Clinical research on microdosing ibogaine is still limited. Recent reviews of microdosing with other psychedelics like LSD and psilocybin found minimal effects beyond placebo in controlled settings, even though many people report subjective benefits in open settings [1]. These findings are one reason professional programs are cautious about presenting microdosing as a proven treatment.
If you want to explore this approach in more depth, you can review ibogaine microdose therapy and ibogaine microdosing benefits for a more focused look at how small doses are being used.
Therapeutic and full flood dose range
Most of the published ibogaine research for opioid detoxification and addiction treatment uses what are often called flood doses or full doses.
In an outpatient ibogaine assisted detoxification program in Mexico, for example, ibogaine hydrochloride doses commonly ranged around 15 mg/kg plus or minus 5 mg/kg, adjusted for weight and the complexity of polysubstance use [2]. In practical terms, that means many participants received doses in the 10 to 20 mg/kg range.
At these levels:
- Sessions typically last 12 to 36 hours
- You pass through distinct phases such as acute, evaluative, and residual states
- Strong psychoactive effects and vivid waking dreams are expected, not accidental
These are not functional doses. You do not go to work, drive, or care for children while undergoing this level of treatment. Instead you are usually in a residential or hospital level setting with monitoring and support, following a structured ibogaine treatment dosing protocol.
For a plain language overview of what this entails, you can visit what is a flood dose ibogaine and ibogaine full dose treatment.
Microdosing vs flood dosing: Purpose and goals
One of the most important parts of any ibogaine dosage comparison is recognizing that microdosing and flood dosing are usually trying to accomplish very different things.
What microdosing typically aims to do
In many psychedelic circles, microdosing is promoted as a way to:
- Support mood, creativity, or focus
- Ease anxiety or depressive symptoms
- Provide a “gentle” path into working with a substance
With ibogaine specifically, some people explore microdosing in hopes of:
- Gradually easing cravings or dependence
- Preparing psychologically for a later full dose
- Avoiding the intensity and medical risk of a flood dose
However, a 2025 research review on psychedelic dosing highlighted that microdosing with other substances has not yet shown strong benefits beyond placebo in controlled trials, while macrodose or full dose protocols have produced more robust and durable symptom relief in conditions like major depression and PTSD [1].
Because of this, microdosing is usually approached as experimental or exploratory, not as an established primary treatment. That is especially true for high risk conditions like opioid use disorder, where withdrawal and relapse carry serious medical consequences.
What flood dosing is designed to do
Flood dose or full dose ibogaine protocols are built around very specific therapeutic goals:
- Rapid interruption or elimination of acute opioid withdrawal
- Substantial short term reduction in cravings
- A psychologically intense experience that often includes insight into the roots of addiction
In the Mexico outpatient study mentioned above, about 80 percent of participants reported that ibogaine at doses around 15 to 20 mg/kg eliminated or drastically reduced withdrawal symptoms [2]. Around half reported meaningful reductions in craving for at least one week, and about a quarter reported reduced craving for three months or more.
Outcomes on long term abstinence were mixed, but still notable given the severity of cases. Thirty percent of participants did not return to opioid use at all, and among this group, over half remained abstinent for at least one year, while nearly a third sustained abstinence for two years or longer [2].
These kinds of results are one reason flood dosing protocols remain central in clinical practice, even though they are intensive and carry real risks.
If you are trying to decide which approach fits your situation, ibogaine microdosing vs flood dose can help you map these goals more directly onto your own circumstances.
Clinical evidence for different ibogaine doses
When you compare ibogaine doses, it is important to weigh actual research data instead of relying only on anecdotes. The available evidence is still limited, but some patterns are emerging.
Addiction treatment and detox studies
In the Crossroads Treatment Center study in Mexico, the 15 mg/kg plus or minus 5 mg/kg dosing protocol did more than just ease withdrawal. Participants who reported stronger psychological insight into the causes of their addiction during their session were more likely to have better treatment outcomes.
Researchers found that while acute subjective effects like the intensity of visuals were not significantly different between treatment responders and non responders, responders more strongly endorsed gaining insight into the origins of their addiction at these typical flood doses [2]. In other words, the quality of the experience seemed to matter more than raw intensity.
Long lasting subjective effects like vivid waking dreams and increased insight were also correlated with better psychological outcomes. Responders showed lower depression and anxiety scores months after treatment, again tied to experiences at around 15 mg/kg plus or minus 5 mg/kg [2].
These findings highlight two key points for your dosage comparison:
- Flood doses in structured protocols can deliver significant symptom relief and psychological shifts
- The therapeutic value appears tied to both pharmacology and the depth of the subjective experience
PTSD, TBI, and mystical type experiences
A secondary analysis of a protocol combining ibogaine with magnesium in male combat veterans with both traumatic brain injury and PTSD found that the intensity of mystical type experiences predicted larger drops in PTSD severity immediately and at one month follow up [1].
In this group:
- Stronger scores on a standard mystical experience questionnaire correlated with bigger clinical improvements
- Those same scores also correlated with changes in brain rhythms, specifically reductions in peak alpha frequency on EEG at one month [1]
This suggests that adequately high doses which reliably produce immersive psychedelic states can create measurable shifts in both symptoms and brain activity, at least in some populations.
Macrodose protocols vs microdosing
Putting this all together, current research suggests:
- Macrodose or flood dose psychedelic protocols, including ibogaine, tend to show more durable symptom relief in serious conditions like major depression and PTSD
- Microdosing across several psychedelic compounds has so far shown minimal effects beyond placebo in randomized controlled trials [1]
Because of this, experts caution against marketing microdosing as a formal treatment before evidence clearly supports it, while at the same time recognizing that macrodose therapies are producing consistent clinical value in carefully controlled settings [1].
From a safety and ethics standpoint, that means structured flood dose protocols in medical programs are more likely to be used as front line tools, while microdosing is approached as experimental or adjunctive.
If you want a structured overview of how different dose levels are applied in practice, ibogaine treatment dosing protocol and ibogaine flood dose experience can give you a more step by step look.
Safety, toxicity, and the risk side of the comparison
Any honest ibogaine dosage comparison must include the risk profile. Ibogaine is not a benign plant supplement. Its therapeutic window is relatively narrow and it can affect the heart in dangerous ways.
Known risks at higher doses
Ibogaine treatment for drug dependence typically relies on large doses that intentionally induce hallucinations. These intense experiences are usually considered integral to the treatment. However, high doses have been linked to serious adverse effects including:
- Ataxia or loss of coordination
- Gastrointestinal distress
- Ventricular arrhythmias and disturbed heart rhythms
- Sudden unexplained deaths in patients, often with pre existing risk factors [3]
Toxicology research in rodents indicates that the oral lethal dose of ibogaine is around 263 mg/kg of body weight. In those same animal models, intraperitoneal doses that were effective in reducing drug seeking behavior also caused neuronal injury in the cerebellum [3].
Researchers who analyzed this data used standard safety factors to estimate what might constitute a conservative starting dose in humans. Accounting for species differences and individual variability, they arrived at a recommended initial dose of about 0.87 mg/kg body weight, which is far below the 10 to 20 mg/kg levels commonly used in addiction treatment [3].
The authors of this toxicology work warned that unless ibogaine dosing is reconsidered and reduced in susceptible patients, morbidities and mortalities associated with its use are likely to continue [3].
What this means for your dosing decisions
These findings do not mean ibogaine has no place in treatment. They do emphasize that:
- You cannot safely treat ibogaine like a typical supplement
- It is unsafe to assume that if one dose is good, more is better
- Cardiac screening, electrolyte management, and continuous monitoring are not optional add ons but central parts of safe practice
Macrodose protocols require skilled therapists, extended preparation and integration, and careful medical evaluation, including heart monitoring, because the combination of pharmacologic effects and psychological intensity is complex to manage [1].
Within this framework, lower dose or step wise protocols that remain within clinically validated ranges may help balance efficacy and safety. A structured ibogaine treatment dosing protocol can outline how reputable programs adjust doses based on weight, medical status, and concurrent medications.
How clinical programs structure ibogaine dosing
When you compare ibogaine dosages across clinics, you will notice some common patterns. These are designed to maximize benefit while reducing the chance of severe adverse reactions.
Weight based calculations and staged administration
Most medical programs use weight based dosing as a starting point, then refine from there. In the Crossroads dataset:
- Ibogaine hydrochloride was typically administered in a range of 15 mg/kg plus or minus 5 mg/kg
- Doses were adjusted downward or upward depending on the severity of polysubstance use and individual risk factors
- Treatment unfolded over 12 to 36 hours, with a clear progression through acute, evaluative, and residual phases [2]
Instead of giving the full flood dose at once, some programs divide it into an initial test dose, followed by one or more larger increments if vital signs remain stable. This allows medical staff to monitor for early cardiac changes or unusual reactions.
Other structured elements often include:
- Strict pre treatment cardiac screening
- Medication review to eliminate dangerous interactions
- Controlled environment with continuous monitoring
- Clear criteria for aborting or adjusting the session
Learning more about the ibogaine dosing methods explained can help you understand how split dosing, booster doses, and test doses fit into the bigger picture.
Why macrodose programs still dominate clinical use
Despite the risk profile and the availability of theoretically safer low dose options, medical ibogaine programs continue to focus on macrodose or flood dose protocols for a simple reason. They are the ones with the most documented clinical impact.
Across different studies and case series, properly screened and monitored flood doses have:
- Interrupted acute opioid withdrawal in a large majority of patients
- Produced at least short term craving reductions in many participants
- Led to long term abstinence in a meaningful minority of cases [2]
In contrast, microdosing has attracted a great deal of interest but has not yet proven itself in controlled clinical trials as a stand alone treatment, whether for addiction or other psychiatric conditions [1].
When you weigh ibogaine dosage options, this is a crucial comparison. Programs that center on full dose treatment are aligning themselves with the strongest available evidence, while programs or individuals that rely purely on microdosing are operating primarily in an experimental zone.
To see how these ideas play out in real world settings, you can review ibogaine full dose treatment and ibogaine microdose therapy side by side.
Choosing between microdosing and flood dosing
The decision to pursue any ibogaine work, and especially to choose between microdosing and flood dosing, is highly personal. It also carries real medical and legal implications depending on where you live.
Questions to ask yourself and providers
As you compare ibogaine doses and protocols, it may help to ask:
- What is your primary goal, for example acute detox, long term mood improvement, insight, or gradual behavior change
- How severe is your substance use, and what is your current level of physical dependence
- Do you have access to medically supervised care, including cardiac monitoring
- Is your provider basing their protocol on published evidence and toxicology data, or mainly on tradition and anecdote
- How will risks like arrhythmia, electrolyte imbalance, or underlying heart disease be screened and managed
A transparent program should be comfortable explaining why they use specific dose ranges, how they adjust for individual risk, and how their approach fits within existing research on difference between ibogaine doses.
Matching dose intensity to your context
In broad terms:
- If you are dealing with severe opioid dependence and life has become unmanageable, a well structured flood dose protocol in a medically supervised setting is closer to what the research supports
- If you are relatively stable, exploring personal growth, and have no urgent withdrawal issues, a cautious microdosing trial within a broader therapeutic framework may be considered, but it should not be sold to you as a proven cure
Either way, it is important to recognize that ibogaine is rarely a stand alone solution. The most positive long term outcomes generally occur when high quality preparation, psychotherapy, social support, and aftercare are integrated into the process.
Using guides like ibogaine microdosing vs flood dose along with the resources already mentioned can help you place your own situation in context and ask more precise questions of any provider you consider.
Ibogaine dosage comparison is not just about numbers. It is about aligning dose, medical safety, therapeutic support, and your personal goals in a way that respects both the power and the risks of the medicine.
By taking time to understand how different ibogaine doses work in the body and in real clinical settings, you give yourself a clearer path to evaluating your options and making decisions that fit your circumstances as safely and thoughtfully as possible.
References
- (Delphi Circle)
- (PMC)
- (PubMed)