Ibogaine treatment dosing protocol can be confusing when you first start researching options. You might see terms like “flood dose,” “test dose,” and “microdosing,” along with very different opinions about what is safe or effective. Understanding how structured ibogaine protocols are designed, and how they differ from experimental or self-directed use, helps you make more informed and cautious choices.
This guide walks you through how ibogaine dosing generally works in medical and retreat settings, what the evidence says about safety, and how microdosing compares to full, or flood, dose treatment.
Understanding ibogaine dosing basics
Ibogaine is a powerful indole alkaloid from the West African shrub Tabernanthe iboga. In Western contexts, it is usually used in relatively large doses to treat substance dependence, especially opioid use. Those large doses are associated with intense psychological effects that many people describe as central to their treatment. At the same time, high doses have also been linked to serious adverse events including ataxia, gastrointestinal distress, ventricular arrhythmias, and sudden unexplained deaths in case reports and series [1].
Because of that risk profile, any ibogaine treatment dosing protocol, whether for addiction or mental health, needs to balance potential benefit against known safety concerns. In more clinical programs, that usually involves:
- Careful medical screening and risk stratification
- Weight based dosing (mg of ibogaine per kilogram of body weight)
- Conservative upper limits on total dose in a 24 hour period
- Continuous or frequent cardiac monitoring in the first 12 to 24 hours
Animal toxicology studies underline why caution matters. In rodents, the oral lethal dose of ibogaine is around 263 mg/kg. When researchers apply safety factors for species differences and vulnerable populations like people with substance use disorders, the calculated initial safe dose in humans is estimated at about 0.87 mg/kg, far below what is used in many current protocols [1]. This gap between theoretical safety limits and real world practice is one reason structured monitoring is so important.
If you want a broader overview before going into details, you may find it helpful to read ibogaine dosing methods explained or the difference between ibogaine doses first.
Key components of a medical ibogaine dosing protocol
Although different clinics take different approaches, there are recurring elements in medically supervised ibogaine treatment dosing protocol designs. These steps are typically used when planning a full flood dose for addiction treatment.
Weight based calculation and dose limits
Most programs calculate ibogaine HCl doses based on body weight. Common ranges for addiction treatment are roughly 10 to 20 mg/kg, often split into an initial test dose followed by one or more larger doses. Reports from treatment centers describe typical “flood” doses around 15 to 20 mg/kg, adjusted for patient weight and severity of polysubstance use [2].
At the same time, safety focused guidelines caution against going too high:
- Doses above 12 mg/kg are associated with more frequent cardiac abnormalities and are regarded as higher risk
- The total ibogaine dose should not exceed 24 mg/kg in any 24 hour period [3]
Extreme body weight can complicate standard calculations. In very overweight or very underweight individuals, some protocols adjust the mg/kg calculation to better reflect digestive system size and to prevent overdosing. Close monitoring of how the person responds to early doses is essential in these cases [3].
If you want to understand dose ranges at a glance, the overview in ibogaine dosage comparison can be a useful companion resource.
Test dose and staged administration
A common safety measure is to begin with a low “test” dose of ibogaine HCl, usually in the range of 2 to 3 mg/kg, at least two hours before the main dose. The goals are to:
- Check for any immediate allergic or idiosyncratic reactions
- Observe basic metabolic response and early cardiovascular effects
- Pay particular attention to those who may be CYP2D6 poor metabolizers, who can accumulate ibogaine or its active metabolite more rapidly [3]
In patients with liver disease or significantly elevated liver enzymes, this test dose becomes even more important. Impaired hepatic metabolism can lead to faster onset, longer duration, or more intense ibogaine effects. In these situations, observation after the test dose may continue for at least eight hours before any decision about further dosing [3].
Some experienced teams argue that with rigorous screening and preparation, a formal test dose is not always required. However, in higher risk populations, many clinicians still favor staged dosing as a conservative safety measure.
Pre dosing preparation and stabilization
Comprehensive programs do not begin full dosing until you are medically and physically stable. That includes factors such as:
- Being well rested and nourished
- Reaching adequate hydration and electrolyte balance
- Achieving a manageable level of opioid withdrawal rather than peak distress
For people detoxing from opioids, some clinical guidelines recommend targeting an Objective Opioid Withdrawal Scale (OOWS) score between 3 and 7 before dosing. If withdrawal is fully expressed, with an OOWS of 10 or higher, dosing is usually delayed to allow for restabilization and symptom control [3].
Specific preparation steps can include:
- Hydration protocols that provide roughly 1 fluid ounce of electrolyte containing fluids per kilogram of body weight, starting the day before dosing and continuing for at least 72 hours afterward, to reduce dehydration and electrolyte loss [4]
- Fasting for 8 to 12 hours before the main dose so that your stomach is empty, which can reduce nausea and vomiting and help ensure that more of the medicine is absorbed [4]
In some research protocols, such as a 2022 open label observational study in the Netherlands, patients on opioid substitution were first converted to oral morphine sulfate for 8 days and then given 10 mg/kg of ibogaine HCl, mixed into yogurt, with metoclopramide beforehand to lessen nausea [5].
IV access and cardiac protection
Because the main safety concerns with ibogaine are cardiovascular and electrolyte related, many protocols build in front loaded protective measures.
Guidelines from the Global Ibogaine Therapy Alliance recommend:
- Inserting an intravenous port before dosing so that IV fluids, magnesium, or emergency medications can be delivered quickly if needed
- Using a preparatory fluid regimen of 1 liter of lactated Ringer’s solution or normal saline plus one ampule of magnesium sulfate, beginning approximately one hour before the flood dose and continuing until about two hours afterward. This can lower the risk of hypotension and protect against torsades de pointes, a dangerous form of ventricular arrhythmia [4]
The 2022 Dutch study illustrates how intensive monitoring can look in practice. Participants received continuous cardiac monitoring with ECGs every 30 minutes during the first 12 hours, then hourly or every 4 hours up to 24 hours. If QTc, a measure of cardiac repolarization, exceeded 500 ms, intravenous magnesium was administered [5].
Despite careful monitoring, this 10 mg/kg protocol still produced a median maximum QTc prolongation of 95 ms. Half of the subjects had a QTc over 500 ms, and 29 percent still had QTc values above 450 ms after 24 hours. These cardiac changes were clinically significant but reversible [5]. The results underscore why full dose ibogaine should not be taken without medical supervision.
Post dose observation and safety window
After a single large dose of ibogaine HCl, the most intensive risk period typically lasts 12 to 24 hours. During that time, structured protocols usually include:
- Continuous 3 lead cardiac monitoring for at least the first 12 to 15 hours
- Close observation by at least one ACLS trained staff member who can respond to arrhythmias or other emergencies
- Ongoing assessment of electrolytes and hydration status in higher risk cases
Guidelines suggest that you remain under supervision until the morphology of the cardiac T wave has normalized for at least one hour. This often happens within 12 to 15 hours but in some people can take up to 24 hours or longer [4].
In addition to cardiac effects, the Dutch study documented severe but transient cerebellar ataxia, essentially significant difficulty with coordination and movement, in the 2 to 6 hour window after ingestion, which generally resolved within 24 to 48 hours. Mild psychomimetic effects were common but usually well tolerated, while opioid withdrawal symptoms stayed low for most participants during the first 24 hours [5].
If you are curious about what this period feels like from the inside, accounts of the ibogaine flood dose experience can provide additional context from the participant perspective.
In medical programs, dosing is not just a single number of milligrams per kilogram. It is an entire structured process that stretches from screening and preparation to acute monitoring and aftercare, all aimed at maximizing benefit and minimizing risk.
Flood dose ibogaine protocols in practice
A flood dose is the high range of ibogaine dosing that produces the classic multi phase psychedelic experience. If you are researching “what is a flood dose ibogaine,” you will often see ranges of 10 to 20 mg/kg referenced as typical.
Purpose and therapeutic goals
Flood dose ibogaine protocols are usually designed to achieve several overlapping aims:
- Provide a “neurochemical reset” for opioid or other substance dependence, including rapid reduction or temporary elimination of withdrawal symptoms
- Induce a prolonged visionary or introspective state that allows you to process life events, trauma, and addictive patterns
- Trigger a window of enhanced neuroplasticity that may support behavior change if coupled with integration work
Observational data from the Crossroads Treatment Center in Mexico are often cited in support of these effects. Between 2012 and 2015, patients there received 10 to 20 mg/kg of ibogaine HCl, with live medical and cardiac monitoring. Most sessions lasted 12 to 36 hours and unfolded across several experiential phases. After treatment:
- 80 percent of participants reported either elimination or drastic reduction of opioid withdrawal symptoms
- 50 percent experienced reduced cravings for at least one week
- 25 percent had reduced cravings for three months or longer
- Around 30 percent were abstinent from opioids at follow up, with many maintaining abstinence for one to two years or more [2]
Notably, treatment responders, meaning those who remained abstinent or substantially reduced their opioid use, also reported more profound spiritual and insightful experiences and had lower depression and anxiety scores at long term follow up. This suggests that dosing and set and setting should not only target physiological effects but also support meaningful psychological and existential processes [2].
You can learn more about the therapeutic aims of high dose work in what is a flood dose ibogaine and ibogaine full dose treatment.
Risks and exclusions
The same report from Crossroads emphasized stringent exclusion criteria. Patients with severe psychiatric disorders, significant cardiac disease, pregnancy, recent use of alcohol, amphetamines, cocaine, certain psychiatric medications, or long acting opioids like methadone or buprenorphine were not accepted into the protocol [2].
Toxicology research adds more caution. High doses that engage multiple neurological receptors and transporters, and which may drive the strong drug aversion response, are also capable of causing neuronal injury to Purkinje cells in the rat cerebellum when given intraperitoneally [1]. Combined with the documented cardiac risks, this has led some authors to conclude that without reconsideration and adjustment of dosing protocols for susceptible individuals, ibogaine related morbidities and mortalities are likely to continue [1].
If you are weighing a flood dose, reviewing a detailed ibogaine flood dose experience and speaking openly with providers about screening, exclusions, and emergency readiness should be part of your decision process.
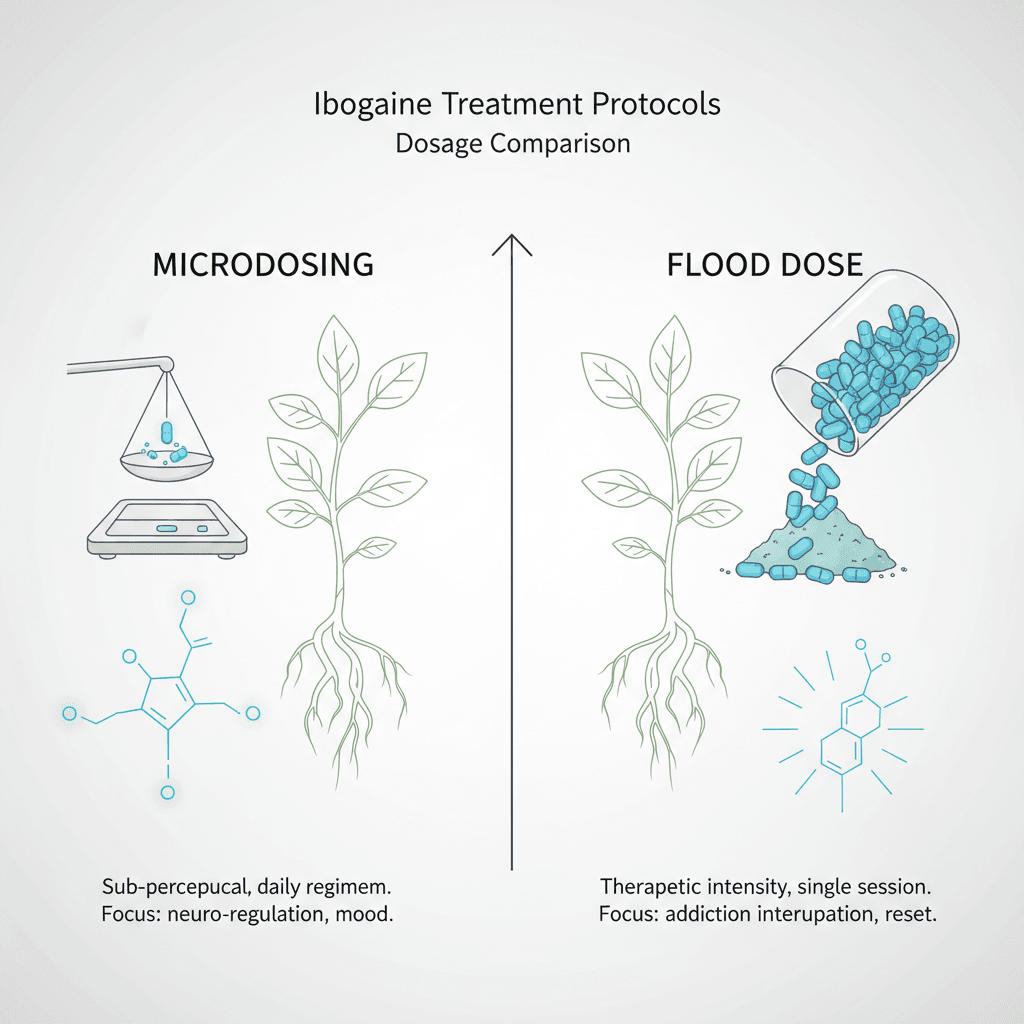
Ibogaine microdosing protocols
In contrast with flood dosing, ibogaine microdosing uses very small, repeated doses that aim to be sub perceptual or only mildly noticeable. This approach is attracting interest both among people in recovery and those with mood disorders, but it is far less studied and carries its own risks.
What counts as a microdose
Ibogaine microdosing is most commonly defined as:
- Doses in the range of 1 to 5 mg/kg of body weight
- Repeated on a structured schedule, such as daily or several times per week
- Low enough that you do not experience the intense visionary or physical effects associated with 10 to 20 mg/kg flood doses [6]
In this framework, the classic flood dose is still considered the primary intervention for addiction treatment, believed to restore opioid receptor sensitivity and drive large scale neuroplastic changes through mechanisms like GDNF upregulation. Microdosing, by contrast, is thought to support ongoing recovery by maintaining some degree of neuroplastic modulation and receptor tuning after the main treatment, rather than replacing that treatment entirely [6].
If you want a focused overview of this strategy, you can explore ibogaine microdose therapy or look at possible ibogaine microdosing benefits.
Example case study: bipolar depression
One published case report describes an ibogaine microdosing protocol for a 47 year old woman with bipolar II depression. In this case:
- She received two capsules of ibogaine HCl containing 4 mg each, twice daily, for 60 days. This dose was approximately 1 percent of a full conventional single dose
- Over time, her scores on standardized measures dropped substantially. By day 15, her Beck Depression Inventory score had decreased by 35 percent, Beck Anxiety Inventory by 39 percent, and Beck Hopelessness Scale by 60 percent. By day 43, reductions were 85 percent, 52 percent, and 70 percent, respectively. At day 90, reductions reached 90 percent, 56 percent, and 100 percent [7]
- She discontinued mood stabilizers and escitalopram on her own but continued alprazolam, and there was no evidence of a manic switch during treatment or follow up. Symptom improvement persisted [7]
Although encouraging, this is a single case, not a randomized controlled trial. The authors highlight ongoing safety concerns, including cardiovascular and vestibular toxicity, and call for more rigorous studies before this approach can be widely recommended [7].
Safety and monitoring for microdosing
One of the biggest misconceptions is that microdosing must be safe simply because the doses are small. Ibogaine, however, blocks cardiac hERG potassium channels at any dose level, which means QTc prolongation and arrhythmia risks do not disappear at lower doses.
Clinics that incorporate microdosing into aftercare, such as MindScape Retreat, typically insist on:
- Baseline cardiac screening with a 12 lead EKG
- Careful review of medications that might also prolong QTc or interact with ibogaine
- Individualized microdose schedules based on a known and stable cardiac baseline, with continued monitoring over a 90 day integration period
- Strong discouragement of self directed ibogaine microdosing outside medical supervision [6]
As of March 2026, there are no published randomized controlled trials on ibogaine microdosing protocols. The rationale for these regimens is based on pharmacology, animal data on GDNF upregulation, pharmacokinetic modeling, and anecdotal reports, while the highest quality evidence still supports flood dose treatment as the main therapeutic intervention for addiction [6].
For a side by side look, the resource on ibogaine microdosing vs flood dose may help clarify which approaches are being used for what purposes.
Microdosing vs flood dose in real world use
When you compare ibogaine microdosing and flood dosing, you are really comparing two different tools that serve different roles in treatment.
Purpose and clinical context
Flood dose ibogaine:
- Is typically a one time or very infrequent intervention
- Is most often used in a residential or inpatient setting for rapid opioid or poly substance detoxification
- Requires intensive pre screening, preparation, and acute monitoring
- Has the strongest evidence for quickly reducing withdrawal symptoms and cravings at least in the short term [2]
Ibogaine microdosing:
- Uses repeated small doses over weeks to months
- Is sometimes used experimentally for mood disorders such as depression or anxiety, and occasionally as an adjunct after full dose addiction treatment
- Currently lacks robust clinical trial evidence and remains largely experimental
- Still requires cardiac screening and attention to drug interactions despite the lower dose [8]
From a protocol standpoint, reputable programs tend to reserve microdosing for aftercare following a medically supervised flood dose, not as a stand alone replacement. That is because the comprehensive neurochemical reset and large scale neuroplastic changes associated with 10 to 20 mg/kg dosing are not produced by 1 to 5 mg/kg protocols [6].
Safety considerations in both approaches
Both approaches share key safety themes:
- Careful dosing based on body weight and health status
- Recognition that ibogaine affects cardiac repolarization even at low levels
- Need for medical oversight and emergency readiness
Where they mainly differ is the timing and intensity of those safety needs. Flood dosing concentrates risk into a single 12 to 24 hour period that requires continuous monitoring, intravenous access, and ACLS trained staff. Microdosing distributes a lower level of risk across many dosing days, which calls for good baseline screening and monitoring over time.
If you are still unsure how your situation fits into this picture, resources like ibogaine microdosing vs flood dose and ibogaine dosing methods explained can help you map your goals to specific protocol types.
Using protocol knowledge to protect yourself
You do not need to design an ibogaine treatment dosing protocol yourself, but understanding the principles behind medical programs helps you ask better questions and spot red flags. As you evaluate options, you might consider asking:
- How are doses calculated for my weight, age, and health profile
- Is a test dose used, and how will my reaction be monitored before a larger dose is given
- What cardiac screening is performed before any ibogaine is administered
- What kind of continuous monitoring will be available during the first 12 to 24 hours
- What exclusions are in place for heart conditions, medications, or substances I may be using
- How will hydration, electrolytes, and nausea prevention be handled
You can also clarify whether a program is offering only a flood dose, only microdosing, or using microdosing as an aftercare tool. Pairing this information with deeper dives like ibogaine full dose treatment and ibogaine microdose therapy can help you align any protocol you are considering with your medical needs and recovery goals.
Ultimately, ibogaine remains a powerful but high risk medicine. The evidence to date suggests that structured, medically supervised dosing protocols, stringent screening, and clear boundaries on who is treated and how, are your best protections if you decide to pursue this form of therapy.